When Your Child Has Transposition of the Great Arteries (TGA)
Your child has been diagnosed with transposition of the great arteries (TGA). This is a problem with the 2 main blood vessels that carry blood away from the heart. These are called the great arteries. The positions of these 2 main arteries are switched (transposed). Other structural heart problems often occur with TGA, most often a ventricular septal defect (VSD). Your child’s healthcare provider will assess your child’s heart and tell you the exact defects they have. TGA is a serious heart problem, but it can be repaired with surgery.
The normal heart
The heart is divided into 4 chambers. The 2 upper chambers are called atria. The 2 lower chambers are called ventricles. The heart contains 4 valves. The valves open and close to keep blood flowing through the heart.
In a normal heart, oxygen-poor blood returning from the body fills the right atrium. This blood flows through the tricuspid valve into the right ventricle. The right ventricle pumps this blood through the pulmonary valve. It goes into the pulmonary artery and to the lungs to pick up oxygen. Oxygen-rich blood returns from the lungs and fills the left atrium. This blood flows through the mitral valve into the left ventricle. The left ventricle pumps this blood through the aortic valve to the aorta to send oxygen to the body.
The foramen ovale is a normal hole in a baby’s heart before birth. It’s an opening in the wall (atrial septum) between the atria. It normally closes a few weeks after birth. If it stays open, it’s called a patent foramen ovale (PFO).
The ductus arteriosus is a normal part in a baby’s heart before birth. It’s a blood vessel that connects the pulmonary artery and the aorta. It allows blood to flow between the pulmonary artery and the aorta before birth. It closes shortly after birth. If it stays open, it’s called a patent ductus arteriosus (PDA).
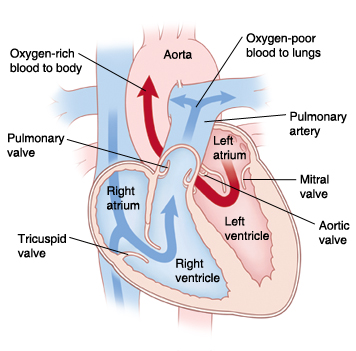 |
| In a normal heart, oxygen-poor blood is pumped to the lungs from the right ventricle. Oxygen-rich blood is pumped to the body from the left ventricle. |
What is transposition of the great arteries?
With TGA, the positions of the aorta and pulmonary artery are switched (transposed). The aorta is connected to the right ventricle. This leads to oxygen-poor blood being pumped to the body. The pulmonary artery is connected to the left ventricle. This leads to oxygen-rich blood being pumped back to the lungs. When a child’s body does not get enough oxygen-rich blood from the heart, this leads to organ failure.
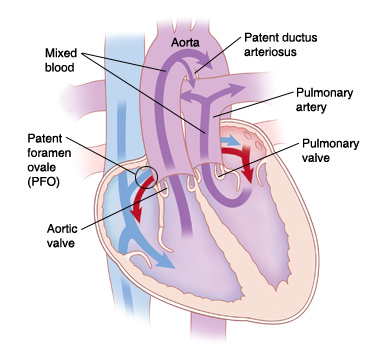 |
| With TGA, the positions of the great arteries are switched. Oxygen-poor blood is pumped to the body and oxygen-rich blood is pumped to the lungs. |
After birth, a child with TGA depends on other heart changes to allow blood to mix in the heart so that some oxygen can reach the body. These may include:
-
Patent foramen ovale (PFO). A PFO allows oxygen-poor blood and oxygen-rich blood to mix between the atria. Mixed blood (blood with some oxygen) from the right atrium can flow into the right ventricle. It can then be pumped into the transposed aorta. Then, mixed blood can reach the body and deliver oxygen. But the blood has less oxygen than normal. Because of this, it may cause your child’s skin, lips, and nails to have a blue tint. This is called cyanosis.
-
Patent ductus arteriosus (PDA). A PDA lets oxygen-poor blood flow from the aorta to the pulmonary artery. As a result, some of this blood can reach the lungs to pick up more oxygen.
-
Ventricular septal defects (VSD). A child with TGA may also have VSD. This may allow for mixing of oxygen-poor and oxygen-rich blood.
What causes transposition of the great arteries?
TGA is a congenital heart defect. This means it’s a problem with the heart that your child was born with. The exact cause is unknown. Most cases seem to occur by chance.
What are the symptoms of transposition of the great arteries?
Children with TGA often have symptoms soon after birth. These can include:
How is transposition of the great arteries diagnosed?
TGA may be found with fetal echocardiography (fetal ultrasound) before a child is born. This test uses sound waves to form a picture of the baby's heart. This test is usually done when the mother is at least 12 weeks pregnant.
If TGA isn't found before birth, signs of a heart problem may be found during a physical exam soon after birth.
If a heart problem is suspected, your child will be referred to a pediatric cardiologist. This is a doctor who diagnoses and treats heart problems in children. Your child may have several tests. These can include:
-
Chest X-ray. X-rays are used to take a picture of the heart and lungs.
-
Electrocardiogram (ECG). The electrical activity of the heart is recorded.
-
Echocardiogram (echo). Sound waves are used to create a picture of the heart and look for structural defects and other problems.
-
Pulse oximeter or oxygen saturation test. The oxygen level in the blood is measured.
How is transposition of the great arteries treated?
TGA is repaired with heart surgery. If your child has other structural heart problems (such as VSD) in addition to TGA, surgery may be more complex. Your child’s cardiologist or surgeon will talk with you about the best treatment options.
Before surgery, newborns are often given medicine to keep the ductus arteriosus open. This medicine is called PGE or prostaglandin. This lets mixed blood flow from the aorta to the pulmonary artery to pick up oxygen.
Your child may also need a cardiac catheterization (cath) procedure before surgery can be done. This procedure is called a balloon atrial septostomy. It's done to widen the PFO until a complete repair (surgery) can be done. During this procedure, a thin, flexible tube (catheter) with a balloon on the end is guided through a blood vessel into the heart. The balloon is inflated to widen the PFO. This lets more blood mix freely between the atria. More oxygen-rich blood can then reach the body tissues.
Risks and possible complications of heart surgery
Risks and possible complications include:
-
Reaction to sedative or anesthesia
-
Arrhythmia (abnormal heart rhythm)
-
Narrowing of the reconnected vessels (pulmonary artery, aorta, and coronary arteries)
-
Heart muscle problems
-
Problems in the lungs
-
Infection
-
Bleeding
-
Problems with the nervous system, such as seizure or stroke
-
Abnormal buildup of fluid around the heart or lungs
-
Death
What are the long-term concerns?
-
Your child may need more cardiac cath procedures or surgery if the reconnected vessels get narrow.
-
After repair of TGA, most children can be active. The level and extent of physical activity will vary with each child. Check with the cardiologist about which activities are OK for your child.
-
Your child will need regular follow-up visits with a cardiologist for life.
-
Your child may need to take antibiotics before having surgery or dental work for some time after TGA surgery. This is to prevent infection of the inside lining of the heart and valves. This is called infective endocarditis. Antibiotics should be taken as directed by the cardiologist.